May
Sports Injuries and Management, Surgical Procedures and Protocols
Wrist Fractures: Causes And Treatments
Wrist Anatomy and Wrist Fractures
The wrist is certainly one of the many complex structures in our body. Given the importance of our hands and their role in facilitating our everyday tasks and activities, it is essential to have your injury and any potential wrist fractures addressed at the onset of your symptoms.
This article will briefly outline some of the common presentations of wrist fractures and give a brief description of how to manage them. It is important to seek the advice and assessment of a Physiotherapist, GP and Specialist to ensure you are receiving the highest level of care.
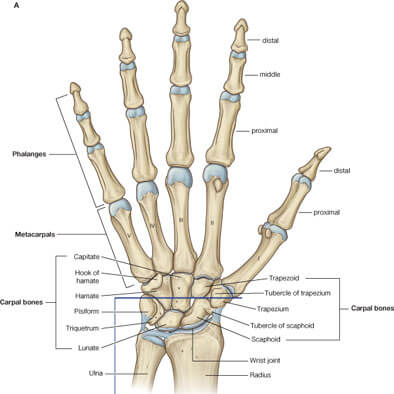
The wrist contains nine small bones neatly joined together by ligaments. This area is commonly referred to as the Carpus. We have two main forearm bones, the radius and ulna, connecting with the wrist from one end. The other end of the carpus is where our finger and thumb bones join (Fig A). We also have a number of tendons and muscles that either traverse the top or bottom of the wrist, some of which extend to the fingers. Accompanying these are nerves and blood vessels 1.
Fractures predominantly occur as a result of a traumatic injury. We typically feel symptoms immediately following a particular movement or mechanism of injury. More uncommonly, we can also experience a pathological fracture. This occurs where you have a condition, such as osteoporosis, that weakens the bone making it more susceptible to fracture. This article will focus on traumatic presentations.
Fracture Terminology
Fractures have many terminologies to describe the stability, placement and bony integrity including
- Stable vs unstable
- Displaced vs non-displaced
- Simple fracture vs comminuted
- Closed fracture vs compound (open) fracture
A stable, non-displaced fracture indicates that the two parts of the bone are fractured but maintain anatomical alignment.
A stable displaced fracture may require re-alignment, but is stable enough to be immobilised in plaster or a splint. If it is unstable, it will require surgical fixation.
A comminuted fracture is when the bone is broken or splintered into more than 2 fragments. These fractures occur during high velocity accidents and are generally unstable.
A compound fracture is a bone fracture resulting in an open wound through which the bone fragments usually protrude 1.
Causes Of Common Wrist Fractures
A fractured distal radius, and/ or ulna can be caused by:
- Falling on an outstretched hand (this type of fracture is commonly called a Colle’s fracture)
- Motor vehicle accident – hands hitting the dashboard / steering wheel / airbag
- Falling on a bend wrist (this type of fracture is commonly called a Smith’s fracture)
A fractured scaphoid usually results from:
- Falling on an outstretched hand. A scaphoid fracture accounts for 79% of all carpal fractures and most commonly occurs in men aged between 20 and 30 years2.
Fracture dislocation of the radio-carpal joint (Barton’s Fracture) occurs from a fall on an outstretched hand. Most of these will require surgical intervention and it isn’t uncommon for the relocated joint to dislocate post-operatively3.
Fracture Management:
When a fracture is nicely aligned, the easiest and safest method of treatment is to apply a plaster (POP) or a thermoplastic splint. The wrist will be immobilised between three to six weeks, depending on the severity of the fracture2.
Some displaced fractures are required re-alignment. This may involve an anaesthetic or a nerve block and the Surgeon moving the wrist in a particular way to better align the bones. This can be achieved without opening up the wrist. This procedure is called “closed reduction” or “resetting the bones”. After this procedure, a plaster or splint will be applied. The wrist will remain immobilised for between three and six weeks, again depending on the severity of wrist fractures and whether the bones have started to knit together or unite2.
A procedure where the Surgeon is required to open up the wrist and insert pins, screws or plates is called an “Open reduction, Internal Fixation” or “ORIF” for short. This procedure generally occurs when there is an unstable displaced fracture that requires metal framework (pins, screws, plates, rods, external fixator) to splint the bones together and re-create alignment of the wrist. Generally, a plaster or half cast is put on and removed by the Surgeon a week later to inspect the wound. Depending on the location and severity of the fracture, the wrist may start rehabilitation around 7 to 10 days after surgery 3.
In relation to the scaphoid, this carpal bone has a poor blood supply, so management can be quite tricky, with prolonged periods of immobilisation in plaster or a splint. Depending on the area of fracture, sometimes the scaphoid is surgically pinned. The aim is to improve the potential healing and minimise the risk of the bone dying and the wrist developing osteoarthritis4.
During the rehabilitation phase, your Physiotherapist will guide you with treatment and exercise to help you restore movement, strength and function to the wrist, thumb and digits. This process may span across a few weeks, depending on the severity of the fracture, the amount of soft tissue damage to the surrounding structures and the period of time for which your wrist has been immobilised.
If you have any questions about your wrist, please consult your Physiotherapist today.
About The Author: Sophie Halsall-McLennan is physio from the Geelong & Drysdale region. She owns Fresh Start Physio has a Bachelor of Physiotherapy from Charles Sturt Physiotherapy, and over 12 years of clinical experience as a Physiotherapist and is registered with AHPRA. She is also a Lecturer at Deakin University.
References
- Brukner, P., & Khan, K. (2009). Clinical Sport Medicine (revised 3rd Ed.). McGraw-Hill, North Ryde.
- Skirven,T., Osterman, A., Fedorczyk, J., & Amadio, P. (2011). Rehabilitation of the Hand and Upper Extremity (6th Ed.). Elsevier. Philadelphia
- Website www.orthofracs.com
- PHILLIPS, T., REIBACH, A., & SLOMIANY, W. (2004). Diagnosis and management of scaphoid fractures. Washington Hospital Family Practice Residency, Washington, Pennsylvania
Disclaimer: Sydney Physio Clinic provides this information as an educational service and is not intended to serve as medical advice. Anyone seeking specific advice or assistance on Wrist Fractures: Causes And Treatments should consult his or her general practitioner, physiotherapist, sports medicine specialist, orthopedic surgeon or otherwise appropriately skilled practitioner.