Mar
Muscle Pain and Tendinopathy
Muscle Of The Week: The Supraspinatus
Anatomy Of The Supraspinatus Muscle
The shoulder is made up of three bones, the scapula, clavicle and the humerus. The ball and socket joint of the shoulder is comprised of the head of the humerus (being the ball part) and the glenoid of the scapula (making up the socket component). The rotator cuff is a group of four muscles that cover the head of the humerus and work to help stabilise the ball and socket joint, playing a substantial roll in keeping the ball and the socket lined up throughout movement and posture changes. The four muscles of the rotator cuff consists of the infraspinatus, subscapularis, teres minor and supraspinatus muscles. The supraspinatus muscle is the smallest of the four, but probably the most “famous” of the rotator cuff. Supraspinatus is located on the back of the shoulder blade, specifically in the supraspinatus fossa which lies just above the spine of the scapula. From its origin on the scapula, supraspinatus travels underneath the acromion (a part of the shoulder blade akin to the roof of the ball and socket joint) on its way to its insertion point at the superior facet of greater tuberosity of the head of the humerus.
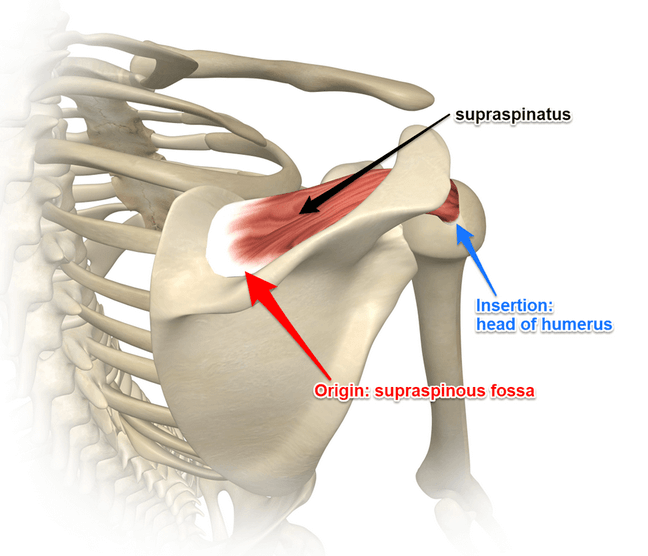
More simply put the supraspinatus muscle comes from the back of the shoulder blade and attaches near the “ball” of the ball and socket joint. Through its origin and insertion points it can act on the shoulder to abduct the arm away from the body. Abduction of the shoulder being the movement of lifting your arm away from your side, supraspinatus is considered to be instrumental in the initiation of shoulder abduction. When the arm is at the side the angle of pull that the deltoid muscle, a power abductor of the shoulder has is not conducive to being able to lift the arm away from the side and needs the supraspinatus muscle to get the ball rolling, initiate the movement which then once the arm is off the side then the deltoid can kick in and take over. Supraspinatus is very much an important stabilizer of the shoulder joint, working the the other rotator cuff and biceps long head tendon to assist in keeping the ball firmly pressed medially against the socket and helps to resist gravitational forces which pull at the shoulder from the weight of the upper limb downwards and contract to reduce migration of the ball superiorly in the socket rising up to compress and impinge tissue against the acromion.
Supraspinatus And The Subacromial Space

Supraspinatus travels from its origin on the back of the scapula through the subacromial space beneath the acromion. Passing between the acromion and the top surface of the humeral head, on its way to inserting onto the greater tuberosity of the humerus. The Subacromial Space measures approximately 1cm when in the anatomical position (arms resting at your side, palms facing forward) and contains a number of structures including the subacromial bursa and the long head of biceps tendon. The subacromial space can become compromised with certain shoulder movements and postures, positions and actions potentially causing impingement (compression) of these subacromial tissues including the supraspinatus may lead to the onset of pain and/or cause damage. Either immediately through traumatic injury such as a fall onto an out stretched arm or elbow, or more gradual onset of change over time with repetitive compression of the subacromial space associated with occupational activities, sports or even sleeping positions (sleeping facedown with arms up under the head).
Assessment Of The Rotator Cuff
The “Full Can” and “Empty Can” special tests are two commonly used examination tests for assessing supraspinatus. They aim to assess the integrity of the supraspinatus muscle and tendon complex and any potential signs of painful impingement of the tendon in the subacromial space.
- With both these tests the arm is positioned at shoulder height in the plane of the scapula (approximately 30 degrees outwards of true forward flexion).
- For the “empty can” test, the arm is then positioned in full internal rotation with the thumb pointing downwards as if pouring out a can of drink (hence empty can).
- For the “full can” test the thumb is pointing upwards (hence the name “full can”).
- Holding the above positions the individual is then asked to resist downward pressure applied to the forearm near the wrist.
- A positive tests result is if there is significant pain and/or weakness.
- The difference between the “full can” and the “empty can” is that the “full can” is suggested to allow more room in the subacromial space and less likely to elicit pain as a result of impingement when compared to the “empty can” test. If pain is experienced with a “full can” test it is more likely related to loading on tendon structures where as the “empty can” positions the shoulder as such that the subacromial space is relatively compromised and pain may be in part related to “impingement”. Both tests load the supraspinatus and a positive “empty can” with a negative “full can” test can indicate the possibility of impingement playing a role in the individual symptoms.
Disclaimer: Sydney Physio Clinic does not endorse any treatments, procedures, products mentioned. This information is provided as an educational service and is not intended to serve as medical advice. Anyone seeking specific orthopaedic advice or assistance on Muscle Of the Week: Supraspinatus should consult his or her general practitioner, sports medicine specialist, physiotherapist or otherwise appropriately skilled practitioner.