Apr
Muscle Pain and Tendinopathy
Spotlight On The ITB And Its Function
What Is The ITB?
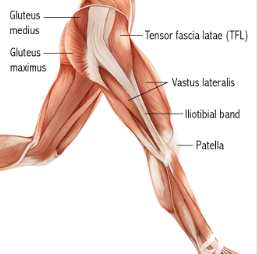
The iliotibial band, sometimes referred to as the iliotibial tract, or the ITB for short is a thick band of fascia (connective tissue). The connective tissue originates from the Tensor Fascia Lata (TFL) and Gluteus Maximus (glute max) muscles on the outside of the pelvis as seen in the image below. The fascia forms a wide band from this origin, traveling over the hip bone along the lateral side of the thigh crossing the knee joint on the way to its insertion. The ITB inserts just below the knee, on the lateral condyle of the Tibia, at a point that is referred to as ‘Gerdy’s Tubercle’.
The iliotibial tract is classified as a deep fascia and is made of dense regular connective tissue, a form of strong and tough fibrous connective tissue made mostly of collagen fibers. Collagen is one of the strongest structures in body and is not very elastic, giving the iliotibial band significant strength in the direction the fibers are running.
What Is The Function Of The Iliotibial Band?
The iliotibial band plays an important role in the movement of the thigh by connecting hip muscles to the lower leg at Gerdy’s Tubercle on the tibia.
- Important in assisting stability of the leg during the stance phase of walking and running.
- Also working to help resist torsional movements around the knee joint.
- Through the TFL and glute max origins the ITB can also assist abduction movement of the hip and thigh.
- Functionally, the iliotibial band helps to extend the action of the TFL muscle into the lower thigh and leg, therefore allowing it to function as an flexor, internally rotator and abductor of the hip and thigh.
- The ITB also allows TFL and glute max muscles to act to support extension and stabilization of the knee and is therefore constantly in use throughout walking and running motions.
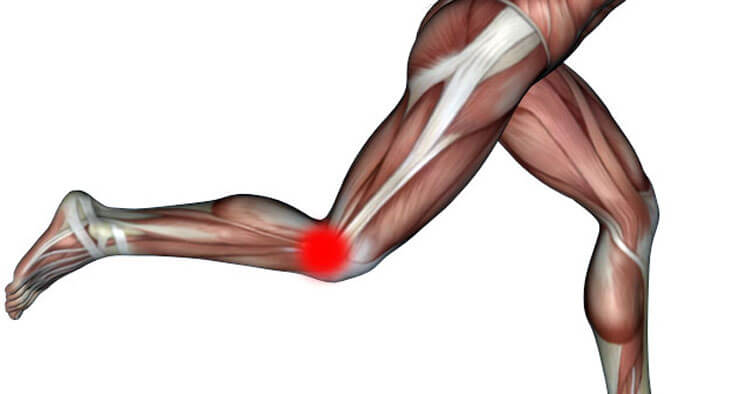
Issues Involving The ITB At The Knee
Iliotibial Band Syndrome (ITBS) is one of the most common causes of knee pain running and in general is one of the most common running injuries we see at our Sydney and Randwick physio practices. As mentioned above the ITB stabilizes the hip and knee during running, and as you run the iliotibial band can “rub” backwards and forwards over bone (the lateral condyle of the femur) and underlying fat pad as the knee flexes and extends throughout the running phases. When this happens repeatedly, as it does with long distance running, the area may become inflamed, causing the band itself and surrounding tissues become irritated and painful. The location of pain with iliotibial band syndrome is felt typically at the outside of the knee, just above where the ITB crosses the joint often at the site of the the lateral epicondyle of the femur and is generally quite easily located as being tender on palpation with individuals suffering with the condition.
With iliotibial band syndrome pain usually occurs just after initial contact with the ground and progressively worsens throughout a run or walk. So at the onset of running the knee may well feel totally fine only for pain to develop later into the run (often after only a short time 1-2km). Following onset, pain may persist unchanged or build to a point where the pain is considerable enough to have the individual stop, or change their running style to avoid knee flexion, attempting to run with a a limp attempting to run with a straight knee. ITBS is often particularly noticeable with long slow running, or running downhills or stairs. With the pain frequently persisting despite cessation of running, felt for a day or two post run when going down hills, or stairs and sometimes simply walking is uncomfortable for a day or two following running with ITBS. It is a condition commonly treated by physiotherapists and multiple approaches can be of benefit including, treatment looking to address strength in and around the hip and knee, mobility work for hip and knee, foot biomechanics and footwear changes, adjustments to running stride and training loads… Managing ITBS pain is not a one size fits all approach and some runners will benefit mostly from strengthening and others from adjustments to stride length and foot biomechanics, our physios are trained in identifying which approach/approaches would best help manage a successful return to running pain free.
Disclaimer: Sydney Physio Clinic provides this information as an educational service and is not intended to serve as medical advice. Anyone seeking specific advice or assistance on Spotlight On the ITB And Its function should consult his or her physiotherapist, general practitioner or sports medicine specialist.