
Jan
Sports Injuries and Management
Management Of An Ankle Syndesmotic Injury
Presentation Of An Ankle Syndesmotic Injury
In my experience the majority of patients having suffered an ankle syndesmotic injury will present with pain in the anterior, or lateral aspect of the ankle, or lower leg. The onset of these symptoms will be following a traumatic incident to the ankle, more often than not the result of an injury during a sporting endeavor. In the chronic situation, or where individuals with acute injuries are still capable of continuing physical activity they may also report feelings of instability in the ankle joint, particularly instability associated with lateral movements, or cutting type maneuvers. Individuals with a chronic ankle syndesmotic injury and instability may have developed symptoms of arthritis at the ankle joint by the time they seek medical attention. Arthritis at the ankle joint resulting from previous injury and continued high load activity over a period of time following injury may potentially be the cause of both ankle discomfort and ankle stiffness. It is therefore not uncommon for individuals who have a chronic high ankle sprain with associated instability of the ankle to have persistent pain, swelling, as well as stiffness and impingement signs.
Patients following an acute high ankle sprain will often report the following symptoms:
- Pain felt above just above the ankle joint, pain which increases when outward rotation is applied to the foot.
- Pain with walking, often there is significant bruising and swelling across the higher ankle area, rather than lower down around the malleolus as is more common with a classic lateral ankle sprain.
As with most injuries, the severity of any symptoms depend on the grade of sprain and individual circumstances. Athletes with a high ankle sprain, without bony fracture may well be able to bear weight on their ankle after injury. However, because miss-diagnosing an ankle syndesmotic injury can result in prolonged disability, assessment and investigations are necessary when any high ankle sprain injury is suspected.
Examination And Investigation Of Ankle Syndesmotic Injuries
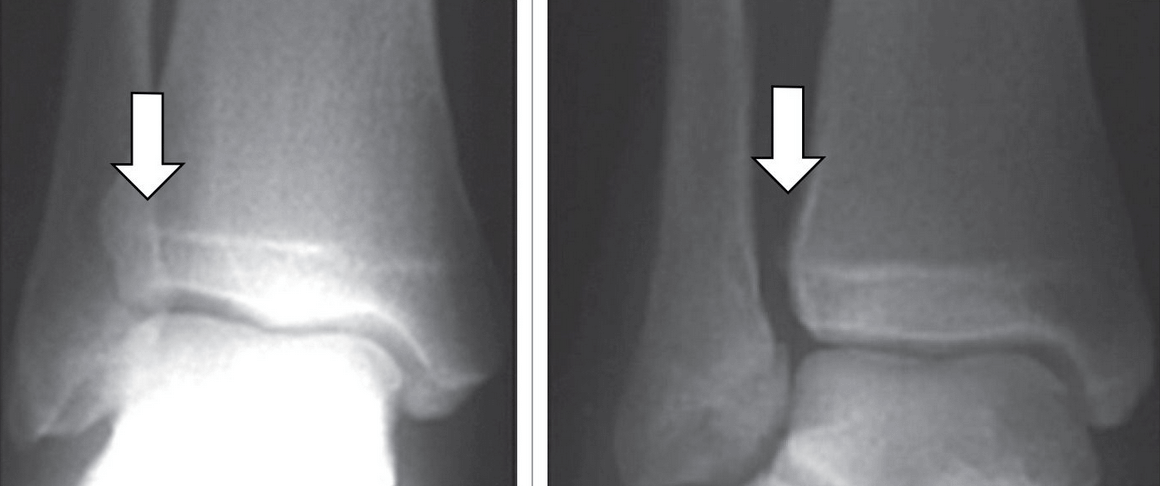
As with most sporting injuries a high ankle sprain is ideally diagnosed early to allow the appropriate treatment to be initiated and accelerate a return to play. If a high ankle sprain is suspected an MRI, or weight bearing X-ray, or CT scan may be ordered to help confirm the diagnosis. With a weight bearing X-ray, gaping at the inferior tibiofibular joint when compared to the non injured ankle is a sign of an ankle syndesmotic injury. Unlike an X-ray, an MRI can visualize ligaments so can detect tears to the syndesmotic ligaments and is a useful investigations with a high ankle sprain is suspected.
Treatment For A High Ankle Sprain
Treatment of acute ankle syndesmotic injuries depends on the injury severity and the stability of the joint complex.
- Grade I injury: Stable injuries can be treated conservatively. Managed with a period of immobilizaiton, protected weight bearing and then progressed with gradual physiotherapy rehabilitation and a return to play in often only weeks post-injury.
- Grade II and Grade III ankle syndesmotic injuries: Individuals will be managed with either a conservative approach as discussed above, with varying lengths of each phase of the rehabilitation. Assessment of high ankle sprains by an orthopaedic surgeon is recommended when there is suspicion of syndesmotic injury and there is instability on assessment. In higher grade injuries some form of surgical fixation where the goal is reduction of the ankle syndesmosis with some sort of internal fixation may be recommended by the orthopaedic surgeon to give the best outcome and enable a return to full per-injury activity .
Disclaimer: Sydney Physio Clinic provides this information as an educational service and is not intended to serve as medical advice. Anyone seeking specific advice or assistance on Management Of A High Ankle Sprain should consult his or her physiotherapist, general practitioner, sports doctor, orthopedic surgeon or otherwise appropriately skilled practitioner.