Dec
Muscle Pain and Tendinopathy, Sports Injuries and Management
Is Plantaris A Cause Of Achilles Tendinosis?
Plantaris Muscle: More Than Just A Hypothetical Cause Of “Tennis Leg”
The relatively common injury of “tennis leg” occurs most frequently during running or jumping activities and is usually the result of an eccentric load being placed across the ankle with the knee in an extended position. The sensation experienced is often described by the athlete as though it feels like they were struck on the back of the leg by an object, such as a ball or other piece of equipment like a racquet. Often so much so that the athlete will look around as if to see who “hit” them. There is some dispute in the wider medical community over the role, if any, that the plantaris muscles plays in “tennis leg”. Tears, or rupture of plantaris are described as one of the possible etiologies of “tennis leg” however the involvement is a source of controversy in the literature.
More recently there has been interest in the role of the plantaris tendon in achilles tendon pain. Achilles tendinopathy sufferers will often note that their pain is more prominent on the medial side of the tendon, about 2-7cm up from the insertion of the tendon onto the calcaneus. This part of the achilles tendon is often referred to as the midportion of the tendon. Any dominance of pain felt on the inside part of the midportion of the achilles has previously been explained to be the result of stress on the calcaneal tendon due to overpronation. However, on this medial side of the achilles tendon runs the plantaris tendon and subsequently it has been postulated that the plantaris tendon may in fact play a role in these symptoms.
Anatomy Of The Plantaris Tendon And Achilles Tendon Pain
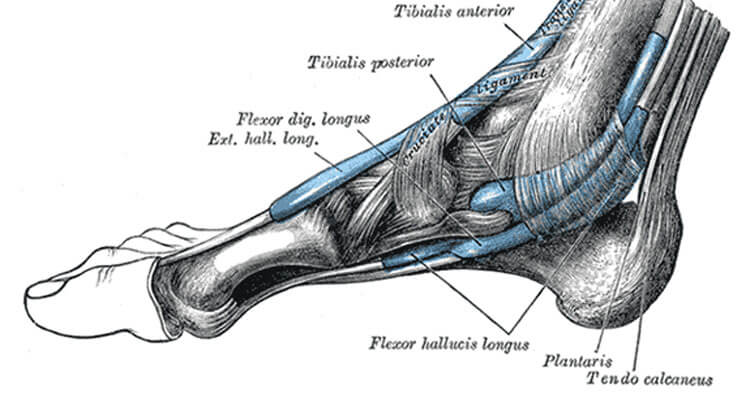
The plantaris tendon travels inferiorly (from top to bottom) along the medial (inside) aspect of the achilles tendon. A path it takes accompanying the achilles tendon to its insertion on the calcaneus (heel bone). In some situations the tendon may insert independently of the achilles tendon and in others it appears to “mesh in” with the achilles on insertion. Differential movement of the achilles and plantaris tendons is one hypothesized account for medial achilles pain. Where abrasion, and adhesions in the tendon have been found in the painful mid-portion zone of the achilles tendon with some sufferers of achilles tendinopathy.
Clinical and histological studies are needed to confirm the role of the plantaris tendon in mid-portion achilles tendinopathy, however some anatomical studies when comparing the material properties of the achilles and plantaris tendons, found plantaris to be stiffer and stronger, suggesting that it could tether the achilles.
The Plantaris Hypothesis As A Cause Of Mid Tendon Medial Achilles Tendinosis
Furthermore some research has suggested a thickened plantaris tendon located close to the medial side of the achilles tendon is common in patients with chronic painful midportion tendinosis. As such this thickened tendon is suggested to increase compression and induce reactions within the cell and matrix and is hypothesised that adhesions between the achilles and plantaris tendons may cause pain by intertendinous traction on sensory nerve fibres.
More Research Required
The role of the plantaris tendon in midportion achilles tendinosis needs to be further evaluated, however should be included in any differential considerations of potential causes of achilles tendinopathy. Literature on proper management for muscular injury of plantaris is scarce, as well as any literature to the role that the muscle may play in functional mechanics. Further research is needed to assess the muscle’s importance to both the mechanics of the calf muscle as well as its any potential role in any other conditions including non-insertional achilles tendinopathy. Considering that it is suggested that non-insertional tendinopathy makes up 66% of achilles tendon pain, unlocking any possible involvement of the plantaris tendon in achilles tendon pain and consequently how best to manage this could be of great benefit to many runners and athletes out there.
Disclaimer: This information is provided as an educational service and is not intended to serve as a substitute for personalized medical advice. Sydney Physio Clinic does not endorse any treatments, procedures, products mentioned in this post. Anyone seeking specific advice, or assistance regarding the “plantaris muscle” should consult his, or her physiotherapist, orthopaedic surgeon, general practitioner, sports medicine specialist, or otherwise appropriately skilled medical practitioner.